I learned more in my 50~+ hours since I got platinum, and a few things changed. A lot is the same, but there’s or altered information.
Preface
BEFORE YOU CORPSMAN!
Coordinate with someone to play shipside nurse.
This will give you time in the beginning of the round to learn about chemistry, the various medicines, and practice level 1 surgery.
You don’t have to, but it’s highly recommended to learn about medicine and treatments in a safe environment.
When I started, I made a text file with the following information:
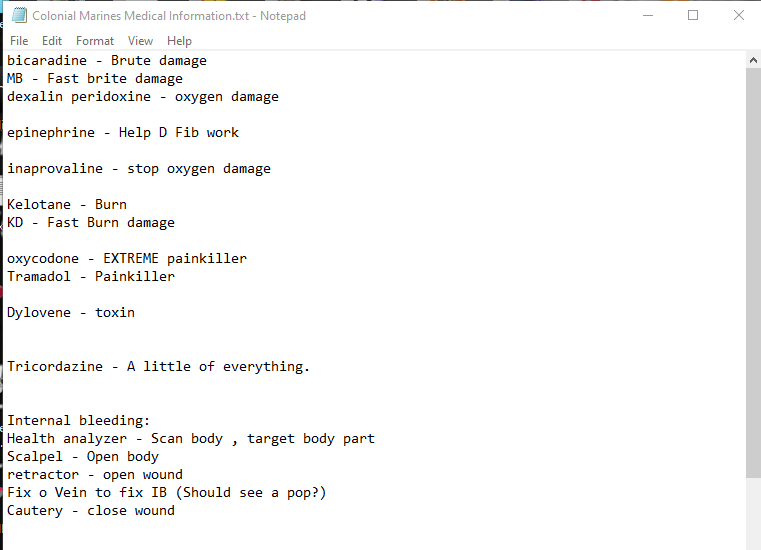

I added information as I felt necessary.
You can check out the wiki too which some medics are able to learn with, but I’m going to teach various techniques and strategies.
TLDR
This is a very long guide.
If you’re new
- Learn medical treatment as a nurse shipside.
- When you treat people, tell them you’re new to medic.
- Bring more splints than you think you should. AT LEAST 5 stacks. 10 or more is better.
- Don’t die.
- Don’t give medicine to marines without checking what medicine they have in them.
- If you’re new, don’t treat anyone else’s patients without reading my section on how to.
- LEARN IB SURGERY!!!
- Ask questions. The best info comes from Synthetics, Doctors, CMO, and platinum medics. There’s still enough dumb gold medal Medics to get incomplete info.
- Take a fire extinguisher
- Bring multiple spare health scanners, and roller beds. You will lose them.
Preface
So if you are considering being a medic, but are skeptical to sink your teeth in, let me tell you about what makes a good medic so you can decide “yeah, a 2.5 hour round as a nurse with 0 patients is something I’m willing to do to learn about being a medic.”
-
Micro.
Medics have the most intense micro-management of any job besides soloing requisitions and certain CIC roles/situations.
You’ll get better at micro, but you’re going to be opening bags, containers in those bags, swapping items around, scavenging gear, swapping hands, and managing other people’s gear with mouse clicks, drags, and keybinds.
If you’re really really scared of messing this up, queue for bravo, as you’re less likely to have added stresses we haven’t talked about yet. Plus Fizz will help you out as a Bravo Corpsman Main for some reason… -
Saving people’s evenings
As we all know, you get 1 life in this game. Games are also 1.5~3 hours which is about all the time some people have after work before they have to go to bed. If someone dies super early in the game, and you can “save their life” it feels so good. In a way you’re actually saving lives as some long rounds can be the only round some people have time for. -
Fighting
If you’re fighting, YOU are WRONG. You need to save the lives of others so THEY can fight. Riflemen fight, Corpsmen heal. Now this is quite ironic because for some inconceivable reason, medics are THE BEST fighters period. It makes no sense, especially since they only have 2~3 mags total. -
Don’t Die
If you die, you are also wrong. Why? Who the fuck is going to revive you? Delta? Don’t make me laugh.
Staying alive is your top priority. If you’re alive, others are alive. You are more valuable than the SLs, and in a metagame, more valuable than the CO, but this is an RP game, so you best be saving the CO. The only person more important than you is the com techs, but you better not die for them.
Avoid fights, or fight to retreat.
Common Fuck Ups
Coming soon… These are just some notes to remind me of what I want to say.
They’re probably not going to make sense to you.
There are a few things Medics mess up on.
-cas evac…
-Reviving mass damage (burns, brute)
-Oxygen (D+ vs Dex, PR, Innaprovaline (In), cas-evac vs roller bed, vs take a hike)
-IB and FE pills (toxins)
Pre-Drop Considerations
Gearing Up
As a medic, you are going to be overburdened with supplies. Generally speaking, optimising how many stupid bulky items you can take is the way to go and there’s a few different strategies in how things are laid out go.
With medical treatment, you’re going to be dealing with your inventory a lot and doing a lot of “micro.” Opening bags, targeting limbs, putting items away to get a different item, etc.
The first important choice to make as a medic is your armor.

This is dictated by 3 factors.
- Damage Resistance.
- Storage Capacity.
- Speed.
Because you’re a medic and can heal yourself, you won’t really need the damage resistance heavy armor offers. B12 is also a type of heavy armor and is not worth 24 points.
But there’s still 4 options.
- Light Armor for speed to get to people, or places.
- Medium armor for 3 storage slots whilst saving on points.
- M4 Pattern Armor for 4 armor slots
- “External Webbing” for ultra-speed, but zero protection.
External webbing is only issued by REQ, and still only has 2 slots as Light armor does.
I’ll make recommendations in the “Medic Speccing” section. These are the important differences.
Next is the Belt. There’s only 2 choices.

- The Medical Storage Rig is the versitile belt.
- The Lifesaver Bag is the large belt.
If you’re a beginner, I recommend the Storage Rig because it can hold nearly every medical item including:
pills, splints, trauma pads, burns pads, defibulators, blood bags, injectors, surgery kits, roller beds, cas evac beds, stasis bags, health scanners, surgical line, and synth graft.
Once you learn to manage your inventory to a more experienced degree, I would recommend the Lifesaver Bag to hold more stuff. It can hold:
Pills, splints, trauma pads, burn pads, injectors, and health scanners.
14 different item types vs 6 different item types.
Though the storage rig can only hold 14 total items, the storage bag can hold 21.
Pouches
Your first one is “Revival Mix - Tricordazine.” It’s the first one in the list.

There’s a lot of solid options for your second pouch.
- Pressure Regents Canister (whatever you want)
- Medical Kit Pouch
- Medical Pouch
- Autoinjector pouch
- Vial Pouch
- First Aid Pouch (refillable injectors, pills, etc)
- Flare pouch
- Large general pouch
- Sling Pouch
- Various Magazine Pouches
I’m going to skip Pressure Regents canisters for now, because there’s a lot of cool stuff to discuss.
2 & 3; The Medical Kit Pouch is a larger version of the Medical pouch, so just take that one. This is what I personally use, and a few other medics use. It’s a 7 slot pouch that doesn’t care about the size of items, only the amount. It can hold:
Health analyzers, droppers, pills, bottles, syringes, splints, trauma pads, burn pads, hypospray, surgical cases, surgical line, burn graft line, roller beds, stasis bags, medevac beds, blood bags, and fixOVein
4 The Autoinjector pouch is also a solid option. Because auto-injectors can be refilled, you can carry a variety of injection based meds instead of using pills to treat your patients.
5 The Vial pouch allows you to carry vials of meds to fill up a syringe. So if you take an extra syringe, you can immediately saturate a patient’s blood stream with the meds you need instead of waiting a couple seconds for pills to be processed.
6 First Aid pouches. The only one I would consider is the refillable injector one because it comes with “!!” or “Emergency injector” which is an instant injection of bicardine, kelotane, tramadol, (maybe oxycodone) that borderline OD’s you as a desperate way to quickly prevent yourself from dying while severely injured.
7 Flare pouch. Flares are one of the least praised items in the game. They let you SEE! YOU ARE NOT LEGALLY BLIND!
If there’s a body in a dark room, tossing a flare or two to see if the body is still there, AND to look for threats is extremely smart. If the front collapses and you’re lurking behind enemy lines looking for just one marine to save, this could be your saviour.
It can also help light up your surrounding area when treating patients. So many medics die from flanks because the marines all push forward whilst you’re still treating patients from the last firefight. 4 or 6 flares can help you see a threat whilst you have a chance to do something about it.
8 Large General pouch. It’s alright. It can hold a few different kinds of items. if you’re fussing with medical and non-medical items, it could be worth it.
9 Sling pouch. A lot of medics like this for their defibulator. No one wants to lose their last good defibulator, so when you do drop it, it jumps back into your pouch so you don’t lose it!
10 Various Magazine Pouches. If you’re still new to being a medic, this could be a good place to keep a few mags whilst you get used to less conventional combat loadouts.
Pressure Reagent Canister Pouches
You already took revival mix… maybe…
There’s a new machine in the Medic Prep room.

It looks like the Pharmacy Chemistry machine, but only accepts Pressure Regent Canisters.

As pressure regent canisters can hold 240~ or so units of medicine, you can customize your own meds including:
- Revive Mixes
- UNGA!!!
- Poison
Epinephrine helps when defibrillating patients.
Tricorzazine helps with burn AND brute damage… slowly.
So one idea is making a mix of Epinephrine, Bicardine, AND Kelotane. This could be dangerous with marines that OD on bicardine and kelotane, but it’s an idea.
I might be experimenting with this more, and and seeing if I can’t make my own is, but this is a really neat feature for those custom regents canister medics that are really advanced with how medicines work in CM.
Webbing
This is the most important choice you will make for what to put on your shirt.

- Brown/Black Webbing Vest - These are great for holding 5 small items, such as: injectors, portable fire extinguishers, splints, blood bags, grenades, health scanners, and shotgun shells.
- Shoulder Holster - Lets you hold a pistol and 2 magazines. Since you’re not fighting a lot, this could be a really solid option for your only weapon.
- Brown/Black Webbing - Really just another good way to hold 3 rifle magazines.
- Drop Pouch - Can hold 2 “square items” and 1 “small” item. People often put Defibulators, binoculars, surgery kits, grenades, MREs, Magazines, and other general items in here. This is now what I personally use, but I might switch to the Shoulder Holster… we’ll see.
This is how “Reid” uses his Drop pouch:

I don’t personally use binoculars, so I put my MRE in there instead.
Helmet
White is Drip. Come at me, Rav. I’m not afraid to choke a bitch!
The regular colour helmet also works fine, but if you lose your helmet, you can always grab an “m10” helmet from the spare armor lockers in your squad’s armory and install a medical optic.

However, to be safe, it’s always advised to grab a medical optic for your glasses from the Wey-Med machines in Lower Medical.

Backpacks
There’s backpacks, and satchels.
Backpacks are really slow and can basically only be used to refill your “main pouches” including your belt, etc. Sometimes I take a backpack not for wearing, but to hold in my hand with extra medical supplies that any medic can take from to refill supplies, like an extra defib, splints, etc.
Satchels are nice because you can treat it like a second belt, and instantly access a defib.
Finally, there’s the radio backpack.
Any of these 3 options are fine. The backpack even on your back can hold a ton of stuff, satchel is fast, and finally the radio backpack is as fast as the satchel but can call people.
I take the radio backpack because when comms are down and I need to do a cas-evac, the only way I can contact the Normandy is to call it.
The radio backpack does provide a burden with specs, bald FTL, and bald SL “needing” you to call people when you’re surrounded by 5 bodies about to perma with 300 burn damage each. Until you can handle it, you’re perfectly in the right to say “no,” “go away,” or “why didn’t you bring one?” If they say “let me just take it off your back” the answer is still “no,” because “I still need my meds if front collapses and we fallback.” Some may persist and say “it’ll be quick.” Don’t lose your supplies and be mean because you told them no two times already. This is exceptionally rare, and only one time did someone try to pickpocket my radio backpack to order more spec ammo.
I label mine, just in case. Sometimes when incapacitated, marines may need it desperately, and borrow it not knowing if I’m KIA.
Treating Patients
Meds
First you need to know your med scanner.

There’s Brute damage which is caused by getting punched, shot, and in rare instances, getting attacked by a xeno’s claws.
There’s Burn, often caused by incendiary CAS, some instances with high explosive grenades like C4, HEDP, flame throwers, exploding ammo boxes, xeno acid spit, xenos acid clouds, some xeno melee attacks. (I hate runners so much…)
Toxin and Oxygen are a bit advanced so we’ll talk about them later.

Here we have the medical mannequin you may be familiar with during your learning nurse round.
Most high brute damage wounds have bleeding.
Between bleeds and burns, bleeding will impose more immediate lasting damages unless burns are drastically higher. IE 130 burn vs 60 brute.
Bleeds must be packed as soon as possible. You could take bandages, but these are simple meds for riflemen. You should basically only use trauma pads, or surgical line.
Trauma pads are instant, stop bleeding, and heal some brute damage.
Surgical line takes a few seconds, depending on the amount of damage, but can heal more damage than trauma pads may. BUT… it never runs out. Trauma pads are at most stacks of 10, and are consumed/destroyed with each application.
Burns can cause oxygen damage. Burns can kill people, but the oxygen can too. Just worry about burns for now.
To treat burns there’s the burn pads, synth graft, ointment, and if you’re really lucky, sometimes someone gives out herbal soothing stuff.
Burn pads are just like trauma pads but for burns.
Synth graft is just like surgical line but for burns.
Ointment is a really crappy consumable like burn pads.
Finally, there’s the herbal soothing stuff. I don’t know what it’s called nor who makes it, but it’s about as good if not better than burn pads. Take it if you see it. Trust me. Verify what heals more damage, but don’t leave it behind.
For some reason treating extreme burns has been made extremely easy. Silver medal medics seem to be able to solo treat 500+ damage no problem, and I have no reason to believe anyone that isn’t a platinum medic read my last guide…
With trauma pads, burn pads, suture, and synth graft, you must target the individual limbs.
The number pad is how you target limbs faster than mousing over individual limbs in the bottom right of the screen.
I bought a “Corsair Scimitar RGB Elite” for $30~USD during the holiday sales, this past winter. Last guide I showed a picture of a razer branded model. Logitech makes something too.

I hate this mouse, but it has programmable buttons like a number pad. It’s pretty difficult to hit a lot of limbs at once, but if you’re dragging a patient, or chasing marines in combat, or quickly tending to wounds, it’s really convenient to not have to move your hands off the keyboard to hit the number pad.
I still use the number pad when treating a patient swiftly, such as a critical marine bleeding on 8 limbs to prevent cardiac arrest.
Finally, there’s fractures. DON’T LET PEOPLE WITH FRACTURES MOVE!
Grab them, if they move, grab them and pull them back to where they were. Disarm them if you must, but generally grabbing is nicer.
If you have to move someone with fractures far, get a roller bed and put them on it-especially if you have to run.
If someone moves with a fracture, there is a chance to cause internal bleeding. People that move with fracs may be new and just not know. Tell them how to check themselves, how to splint, and maybe give them a couple (2-3 max) splints if they didn’t bring any.
I’ve scanned a marine, the marine got hit again without moving and then scanned a second time and he had a frac. He moved 1 tile, and I scanned a third time. Now he had IB. DO NOT let them move IF you can help it.
Some marines can walk 50 tiles and not get IB, so it’s really a gamble that can make you lose hard.
Acid, and the 9 tile circle acid thingy can destroy splints applied to a limb.
As a medic, if you have splints, don’t stick around for your splints to melt. If you can see a doc, or Synth ASAP to get your bones fixed, it can be worth because you cannot waste your splints. Medevac is a last resort if you have like 4 fracs, but ONLY if there are other medics still alive.
Toxin And Oxygen
Aside from listening to me yell at you for leaving your mats in FOB as a bravo com tech at the front with a flamer and 4 slot rifle mag pouches that can’t build cades with an active queen, toxins come in a few forms.
- The brown cloud
- neuro toxin
- overdose
- malicious intent
The brown cloud toxin is annoying but one of the shortest-term toxins.
D+ USED to fix this problem IF you used an Injector immediately. I’ve been experimenting with a Syringe and Dylovene, but I don’t think that solves the problem either. I’ll have to experiment more and perhaps try Dex injections. For now, just stay AWAY and keep victims safe.
Neuro toxin can be delivered to a marine from a xeno from range, or melee. Sentinels and some T3 cause toxin, but it’s not like you could single out one over another anyway to do something significant enough about it.
The only thing you can do is give Dylovene.
Overdosing is usually caused by new medics. Some riflemen or non-medically trained FTL/SL cause self-inflicted overdoses.
Most but not all pills and injections have about 15 units of medicine.

Here you can see I injected myself with tricordazine.
Before you give ANY meds, scan the patient to see what they have in them.
If you revive a patient, or a patient takes a pill, it can take up to 5~10 seconds for the medicine to show up in the bloodstream, and therefore the scanner.
When in doubt, wait 5~ seconds and scan a second time. If ANY medical-looking personnel come near your patient, until you know which medics you can trust, don’t risk an overdose.
Most but not all overdoses happen at 30 units of medicine. Oxycodone, I’m quite certain is one of those meds. Some medics WILL “double dose” some patients to stay under the OD limit, but to treat highly damaged marines. A marine 15 units of medicine over the OD limit is very likely to die. Don’t dose without checking the current dose.
Dylovene will help reduce toxin damage caused by Overdosing by thinning out the meds faster in MOST instances. NEVER double-dose Dylovene. All you need is a marine to have 60 units of dylovene in them…
If you’re at the FOB or almeyer and there’s a dialysis machine, you MUST monitor the patient. Portable dialysis machines have a rechargeable battery and can run out of batteries when treating a patient. ADDITIONALLY… it sucks the blood out of the patient, so you MUST give a steady stream of blood in order for the patient to not die of blood loss on top of an overdose.
This is one of the only ways to treat a Dylovene (anti-toxin) overdose.
Many Dylovene OD patients are as good as perma, but you have to try and help them and it’s a very demanding process to get such a marine back into good shape.
The best treatment for OD is to only give single doses AFTER being absolutely sure no one gave medicine, and telling other medics to leave your patient alone.
Finally, there’s malicious intent. Some chefs, clf, bad marines, etc will poison things like food. Call for MPs, and give dylovene. Bring the patient to medbay.
Oxygen Specific
Oxygen damage is caused by burns, pain, suffocation, lung damage, blood loss, certain drugs, and unknowns.
With burns, if you just treat the wounds, oxygen should go down.
Pain inflicted oxygen damage either needs the wounds treated or some painkillers. I recommend Tramadol. Marines can get Tramadol too, so make sure they didn’t take any already.
Suffocation is often caused by various gasses including the brown cloud xenos make.
Lung damage is caused by Friendly Fire, usually when someone is using armor-piercing ammo.
Lung damage is ALSO caused by CHEST FRACTURES, Including MOVING WITH CHEST FRACTURES.
Not everyone who has a fractured chest has lung damage.
If someone has lung damage, you’re going to find out really quickly.
Some drugs including Oxycodone cause mild oxygen damage. Don’t worry about it. It’s like 4~7 at most and will go down.
Sometimes oxygen damage is caused by things you cannot tell what it is. Is it an unknown toxin? Is it lung damage? Is it a bug in the code? Is it pain? Sometimes when you revive people, they just get a ton of oxygen damage for no reason.
How do you treat Oxygen damage?
First, when you are reviving someone who died, don’t even look at the oxygen damage. After you revive them, it will 99% of the time shoot to 0. Sometimes if you scan someone 5~ seconds after defibbing them, they can have around 13~15 oxygen damage. This is common, and not a major concern.
First thing’s first. Dexalin. This is your pill Dx. This will prevent the oxygen damage from going up.
Next is In, or Inaprovaline. This is related to, but not the same as Ia (I forget the long name… inna and alkysi?)
In will lower the oxygen damage. Patients can pass out from oxygen damage.
Often Pr or Peridaxon is given too as it can heal some minor organ damage.
If someone has over 40 oxygen damage, it’s likely they have lung damage. Some patients can have 38~ oxygen damage but not have lung damage. Over 40, almost guaranteed lung damage. Give Peradoxin, and send them for surgery, cas evac most preferred.
D+ is very helpful as it instantly brings oxygen down to 0. I used to take D+ pills, but now just find myself adequate 95% of the time with my 3 injections. You can always loot another one should you require it.
I have used D+ on just about every common class. The decision comes down to, how quickly do you need this guy up?
Scan and rescan marines with oxygen damage to assure oxygen damage is going down. Sometimes oxygen damage will creep up slowly. Sometimes you’ll defib a patient, and like most, not get up for a bit, BUT… will develop intense oxygen damage with no readable cause and it’s not lung damage. Worst comes to worst, put him on a roller bed and monitor him whilst you treat other patients.
If you give a marine Dx, and tell him to go alone to the FOB to get his lungs fixed, he WILL pass out. It won’t last long enough to stop the oxygen damage from making him pass out, even if you double dose. Medevac, roller bed to FOB, or hand to a Level 2 surgeon. (Doctors, Synths.)
Finally, CHECK BLOOD… some marines really need blood and it’s uncommon but happens where marines will have 40% blood and just pass out and die even thought they aren’t bleeding, even internally.
Make sure you have your two blood bags in your basic kit at the least.
Internal Bleeding
Some medics take the surgery kit and it is the fastest way to treat bleeding with only level 1 surgery skill.
You must remove armor on the limb with IB. hands and feet can be treated without removing armor. Arms, legs, and chest need the main chest armor removed to treat. Helmets must be removed for heads.
If the patient is wearing a hat, headband, or yellow safety vest, you don’t have to remove the clothing.
You can ditch the surgery kit and use your boot knife to make an incision and hold the incision open. Then you can use your surgical line to treat the IB, and then use the surgical line again to close the surgical incision and finally and bleeding that may have occurred.
It can often be useful to transfuse blood as you’re doing IB surgery.
I recently started deliberately not giving blood if the patient has 80% or more blood, and sometimes even 75% blood as some IB and treatments don’t need transfusions.
If you have a patient that has IB, DON’T YOU DARE SEND THEM TO A DOCTOR OR FOB. Some medics do this and it’s pure laziness. A patient with IB can easily pass out somewhere in the backlines and perma. Doctors often have more important treatments to tend to. Many riflemen can handle their own wounds whilst you do a quick IB treatment.
First thing’s first. Verify if they have Tramadol in them (7 units should be enough). If the patient doesn’t I recommend giving a tramadol pill first. THEN put the patient on the roller bed, then go to somewhere safe, then remove the armor, and start the surgery.
Pills as you remember take a couple seconds to take effect.
Never treat IB on the front front.
Stay at least 1 tile behind a barricade with your patient the same.
If there are no barricades, make sure you cannot be flanked, ganked, or otherwise even hugged. All you need is to be slicing the patient when you get hugged and causing more intense damage in addition to the existing IB damage. You know you’re the only one taking yourself back to FOB for an abortion.
I recently started taking the Oxycodone with me onto the battlefield as an instant painkiller injection that doesn’t need me to worry about ODing the patient on tramadol just as another option, but I’ve yet to actually use it as CO’s will automatically stun you for trying to inject them with it.
Because the surgery kit fits in armor slots, I am probably going to start taking it because of how much faster it is for treating IB.
Reviving the Dead
Brute and burn damage are the only two damages that matter.
“revivable” is when the addition of these two numbers is a maximum of 200.
The defibrillator heals some damage, and “revival mix” injections help heal more.
It’s possible to defib some patients with 240~ total burn brute damage and have them live.
There’s a few important symbols to know.
Red and white skulls are permanently dead. A “broken heart” needs to be brought to a doctor or synth to have fixed.

This red flat line is DNR or Do Not Resuscitate. People can go DNR at any point when dead which is incredibly annoying. Some players DNR on death as an RP thing, others will wait for you to spend 2 HEDP, drag them back 10 tiles, treat half their wounds, and pull out your defib to revive them. Unless it’s a smart gunner, spec, or medic during high pop, stop treatment immediately so you don’t waste supplies. Once a DNR sg, spec, or medic is revived, send them up on medevac or cycle in the alamo so the shipside doctors can put them in cryo and a new one may spawn.
Green jagged lines are recently killed.
Flashing orange lines are close to becoming permanently dead. The faster the flashing, the closer to perma.
In most cases, it’s best to check the damage of the patient before doing any treatment as the defibrillator can cause heart damage every time it shocks the patient.
Some marines have a ton of damage on them. If it’s over 400 in one category, you’ll need to treat before reviving.
Not all medics know, but you can treat patients while the defibrillator is charging to shock. It’s quite reasonable to have a patient with 260 damage and defib immediately. whilst the defib is charging, you can treat the wounds of the patient. Splints can only be applied whilst defibbing if you do it immediately, like same frame as you do the defib. Otherwise, when the defib finishes, it’ll stop the splinting. I don’t bother splinting when defibbing because I’m not even sure if you can finish applying the splint if you start splinting on the same frame you start defibbing.
If the patient is still green lining, or just turned orange, and has less than 200~ damage total, treat the IB before reviving IF the front line is guaranteed to hold. It’s faster, doesn’t require tramadol, and the patient cannot lose any more blood because the heart isn’t pumping it out of the body.
If the patient has already started orange flashing before you arrived, it may be best to defib first so the patient doesn’t perma.
With extreme damage, like 600 burns often caused by CAS, if you are by yourself, the patient is most likely going to die unless you start treating them whilst they’re in the green. Call over other medics, and scan patients not being defibbed nor IB treated.
Many medics use the Surgical Line and Synth Graft to treat these wounds as they can treat the most damage per limb, however, it’s also slow.
The fastest way to treat such patients is to use the suture line & burn graft NOT to use trauma and burn pads. With extreme damage, you can apply a kit to the same limb 2 times and in rare cases 3 times in immediate succession. However, the suture line & burn graft does more damage overall in a short period of time. If you use pads, you will treat damage faster, but you will treat less damage overall.
With major damage, it’s also common for a limb to allow treatment to itself again after a short period of time-this may be specific to trauma and burn pads, however.
Unless the patient is really close to dying, and the damage is close enough based on your personal insight to how much damage you can reduce to get closer to the 200 damage sum threshold, stick with the surgical line & burn graft.
Finally, we get to defibbing.
Always inject Revival Mix to your patient, remove the armor on the chest, and apply the defib.
Make sure you remove the paddles to defib, and re-apply the paddles to put it away.
When patients are flashing orange quickly, just start defibbing. It heals damage, and it can break the heart of the patient, but that’s less of a concern compared to a patient going perma because there’s a higher chance the patient will live from “defib spam.” Nearly perma marines are to me at the least, considered already dead, so any risks are unimportant including extremely low blood as resetting the perma timer is more valuable.
When you get better at your micro, watch out for marines with dark red bars flashing normal red.

These are patients close to death, and can be saved from dying by applying trauma pads and burn pads to their wounds on their limbs. It’s more effective than giving pills, though injections may work too; pads are a more likely guarantee of the patient’s living because you can treat a lot of damage instantly.
Eschars & Burn Damage
Eschar burns are a new addition to the burn damage system. Eschars are a type of burn that is so intense that affects the flesh under your skin & you effectively have internal burns.
Eschars on hands and arms can cause marines to drop items unintentionally. If there is an eschar on a hand or arm, it’s best to try and treat it so a marine doesn’t drop his rifle whilst breathing the exhale of a Lurker.
The “correct” way to treat such an injury is to open the limb as though you were treating internal bleeding, but using the Burn Graft to treat the eschar.
Alternatively, if you can get the burn damage to 0, the eschar goes away.
Finally, randomly, Eschar may go away from treating the would from the outside, or otherwise giving Kelotane which may treat the wound from regular bloodflow and the body’s blood vessels taking the Kelotane to the would internally.
Keep in mind, my experience with Eschars is limited, but based on some experimentation, these are the results I was able to deduce.
Collaboration
Support Staff
This is a TEAM game. There are people you CAN rely on. (sorta… it’s still CM13…)
First and foremost is CAS/CASEVAC/Medevac/Normandy.
This is the grey dropship, sometimes called Dropship #2. It is often, but not always manned. 175+ players, you’re basically guaranteed Normandy to be operating.
Normandy’s pilot is often referred to as the “Gunship Pilot” and he has access to the “Medical” radio channel. He also has a phone in his ship. If you have a radio backpack, you can call him like so, and talk normally into the phone with it in your hand.

There’s a lot of downtime for gunship pilots, so the good ones are all very responsive on comms. The most under-used and under-valued use of the gunship pilot is CAS-Evac.
Yes, most hugged marines do get cas-evacced…
But when the FOB falls and you can’t get to the dropship, calling the Normandy, from the last cades available, or really far away from the Opposing Force, you can be extracted without going to the other landing zone which could be an ambush.
Next are Doctors, and Synths.
These guys can do the level 2 surgery. This includes fixing internal organs, mending fractured bones with “bone gel” and aborting hugged marines before they burst. Be nice to them or they might have “just ran out of bone gel… like … just right now… when you asked…”
Under-utilized are the common marines. A lot of hurt marines have a lot of damage, and can’t be deffibbed until the damage has been reduced. yell out “CPR!” and marines may come and give CPR to your patient. Only one person can do CPR at a time. Some attentive marines can be pointed to whilst you’re treating a patient and they’ll know to give CPR.
Finally, and most importantly are the other medics.
You need each other, you can work together. You can save marines faster. But there’s a way to do it.
Treating Patients of Other Medics
NEVER EVER GIVE ANY MEDICINE TO THE PATIENT OF ANOTHER MEDIC.
EVER.
Medics can be caught up in micro and not even see you approach their patient.
I personally wait until after I have treated the patient to decide whether or not I will give any meds.
Other times I will give pills sometime during the treatment. I could have just give the patient a pill when you scanned to see that there’s no drugs in the patient. Maybe I gave a double dose. Maybe the patient had 7 units of a drug, and I bumped them up to 23~, and now if you give another 15 units, they’re at a near 40 unit OD and can pass out and get capped.
Do not give medicine to the patients of others.
If you see a medic over a patient and not defibbing, get a scan.
If the patient is within reasonable defibbing range (300~ damage, green line, or slow flashing orange), walk away so the medic knows you’re not giving any meds, or strip the armor.
If the patient has fracs, immediately show the splints in your hand to show you are only splinting.

It’s common courtesy to splint from bottom to top if it’s not your patient, as most medics treat patients from top to bottom.
Then leave. Go away. Give the medic his space.
If a big battle is going on, just stay away from others’ patients entirely as there’s plenty of other marines that could use your treatment. Most medics can treat most patients by themselves even if they’re a little slow.
When it comes to high-damage patients that a medic asks for help with, or you see 400~600 damage on a patient, don’t inject revival mix without permission, and don’t “steal” their defib.
When it’s close to defib time, and the “first” medic on the patient hasn’t pulled out their defib, say “defib.”
If the patient is starting to get close to rapid orange flashing, and there’s still like 400 damage and you can’t apply burn pads to the patient, it’s polite to ask “defib spam?” and get a yes or no. If the patient is really flashing a lot, just do it and everyone will defib spam. You might accidentally steal a defib which sucks, but sometimes you take them to prevent a marine from going perma.
If someone is treating IB, and the patient has really low blood-less than 50%, it’s okay to help transfuse or ask the medic if he needs blood to help transfuse.
Finally, the only time you can “steal” a defib.
IF a patient is 300+ damage AND is quickly flashing orange AND cannot be quickly padded with trauma nor burn pads… then you whip out your defib and do “defib spam.”
This is when you rapidly use and re-use your defib to try and save the patient.
It is very likely the patient will die, so this is a last-ditch effort to save him, even if it means breaking his heart. Continue treating with your off hand what you can with sutures, and burn graft, but don’t stop deffibbing until he’s alive.
Internal Injuries
Marines can suffer from various internal injuries with various side effects.
Blindness - Caused either by low blood, damaged eyes, or brain damage.
If low blood, give blood until about 70~80%.
If eye or brain damage, give “ia”
Dropping items - Caused by broken hands, broken arms, missing hands/arms, or brain damage.
If broken, add a splint.
If missing, send the patient to the FOB doctor, or the almeyer to get a prosthetic.
If brain damaged, “ia”.
Oxygen Damage - If not caused by an above issue, this could be caused by a punctured lung.
If a lung is punctured, the patient will need lung surgery by a proper doctor.
This can be caused by moving with a fractured chest, rarely being stabbed in the chest, and also being shot by teammates.
“Heartbreak” symbol on a dead patient - The heart is broken. you CANNOT defib this person to revive them. They MUST have heart surgery IMMEDIATELY in order to be defibrillated. They will die without it. The cardiac arrest timer doesn’t stop nor slow down.
Toxin Damage - Often caused by taking too many meds. The kidneys or liver are broken, and need to be healed. This can also happen from being shot by teammates. This can also happen from a fractured groin puncturing the organs.
Treatment requires kidney and liver surgery.
Fractures can be “fixed fixed” by doctors and synths with bone gel. This restores them back to new-unlike splints which just prevent damage.
Additionally, there are some drugs often dubbed “Bone mend” that research can make.
ITEMS PART 2
Spares and backups
I deploy with 2 health scanners. In the beginning I used to deploy with 3. They’re small, sometimes accidentally go into backpacks and armor on the ground when you mean to scan someone, and q is a really easy key to press.
I also take 2 roller beds. Xenos love to hit your roller beds. One hit and it’s gone.
Same goes for the case evac bed, but I just make sure I only do cas evac inside barbed cades, or under really good security. A second roller bed also helps for FOB fallbacks. If you got 5 patients and the rav winks at you as your SL gets decapitated, close the cades, and shout at the last rifleman standing. You gotta save who you can save, and if you can only save one marine, so be it… but if someone else can drag another marine on a roller bed, that’s even better.
D+ is useful for fallbacks, and so are painkillers. You’ll know when you know.
Also… it sucks, but sometimes you have to let go of a roller bed with someone barely clinging to life in order for you to escape. It sucks so much, but it’s sometimes the only way. and if you get somewhere safer and find another downed marine, having the second roller bed will at least save one marine.
Common Meds
You should already know your basic meds. This would be your pills, the suture, the graft, and trauma pads, and the burn pads.
There’s a lot of ways to carry these. The belt is your main storage compartment, but you’re probably going to run out of something.
Many medics carry spares in their backpack in “kit boxes”.
This is what my current backpack loadout looks like:

I’ll cover what I carry in more detail in the “loadout speccing” section.
Custom Meds
The Pharmacy Line is part of your preparations.

During low pop, don’t expect nurses and doctors to be able to make everything. (lowpop is less than 100 players.)
The most important custom pill is Ia.
This pill cures blindness, and brain damage. You must take this pill with you.
Com techs and leadership sometimes forget their welding goggles when repairing barricades.
Various head trauma causes brain damage forcing marines to do actions they don’t intend and other bizarre effects.
MB and KD are popular choices as well.
Meralyne Bicardine is the same as Bicardine but more powerful with the Meralyne.
Kelotine Dermaline is the same as Kelotane but more powerful with the Dermaline.
D+ is something we discussed earlier. I used to take this in pill form. Perhaps the mechanics changed in such a way where I no longer feel it’s necessary, or I got better to not need it.
FE, otherwise referred to as Iron. (FE being the abbreviation for the Latin name on the periodic table of elements.) This helps with blood regeneration. when a patient is alive and low on blood, give them FE to help them regenerate blood. Patients must be alive for drugs to work.
Finally, there’s spaceacillin. This is a very uncommon drug to need. If marines catch the flu, you’ll need this to cure it.
Non-Medical Items
Some non-medical items are really good to have.
Binoculars can be used to get situational awareness, for example if you just revived a marine, and want to see if the front it falling to decide "Should I roller bed this marine for an FOB retreat, or should I go help treat more marines?
HEDP-sometimes referred to as “Meat Hooks.”

The best strategy is to throw or shoot an HEDP one tile past a dead teammate.
The blast will push the body a few tiles away from the grenade blast making it easier to recover bodies in unsafe areas. I don’t know if Julian Vestiel Mao invented this technique, but she is the one that taught most medics I know learned the technique from.
The radio backpack. We discussed this earlier in the backpack section, but when comms are down or you need to talk to someone, it helps a lot.
Normandy for cas evacs,
Alamo for cycles,
medical reception to request FOB Doc, meds, etc,
your squad’s overwatch when you need help recovering bodies or when op is FUBAR, etc,
sometimes req for ammo, metal for com techs to cade, etc.
The boot knife. Instead of taking up valuable space with the surgery kit, you can ignore the scalpel, and retractor. Use your boot knife to make incisions for IB, and hold the incisions open.
Finally, extended mags. You don’t have space for 3 or 4 mags like common troops do, so grabbing 2 extended mags is your best chance of having ammo.
Combat
Defending yourself
We talked about just a few medical supplies… medical treatment, and all this stuff.
Where are you going to carry your guns?
What do you even do with guns?
If you’re starting out, I recommend taking extended m41a magazines if that’s what you’re used to, and keeping them in your armor slots.
Magnetic harness works fine.
1 mag in the gun, 1~2 in your armor. You shouldn’t really be fighting, but you may be forced to.
For more advanced medics ready to carry more medical supplies, we have a few things we can discuss.
- Shoulder holster.
- M39 SMG Holster Rig and Pouch
- M276 Pattern General Pistol Holster Rig
- Smart Pistol
- Unarmed
First is the shoulder holster. It fits on your shirt, and you can get 3 mags. Nice and out of the way.
Allegedly… there’s a pouch that can fit in your armor gun slot. I thought it was the large general pouch but it didn’t work for me, so this could be a myth, or a different pouch.
M39 SMG holster rig and pouch. This fits in the armor gun slot. This holds the M39 SMG (with attachments) and two spare mags. I personally use this and have 3 extended mags total. 1 in the gun, 2 in the pouch.
Pistol holster rig and smart pistol. I never used the smart pistol but I hear it comes with a holster that fits in the armor. The main pistol holster rig holds way more mags than a shoulder holster, so you can use a pistol as your gun if you want that.
Finally is unarmed. I don’t know anyone that plays medic that goes unarmed, but this one shirtless dude in Charlie plays rifleman called “kamikaze” and basically just roller beds downed marines to medics.
If there is a pouch that fits in the armor slot, it could be worth it to you to give up on guns and just take more meds.
When you fight, fight to retreat 90% of the time. If you are on your last mag, use it to refill your mags, or replace your spent mags. DON’T LOSE YOUR EXTENDED MAGS UNLESS YOUR LIFE DEPENDS ON ABANDONING THEM! Req often sends down regular-size mags or loose ammo. The SMG kinda sucks, so you really need all 72~ rounds over the 48~.
Because you’re less likely “in the fight” fighting, a magnetic harness isn’t as necessary as it may be for riflemen.
But now… you better not lose your gun.
Holster your gun in anticipation of a stun/knockdown attack. Even if a hook grab comes, put your gun away. If you get grabbed and killed, if the marines recover you, and lose the control they had over the position you lost your gun at, it’s gone. Good luck finding another SMG or smart pistol, and even then, it’s likely the gun was sent by req unloaded without so much as a bayonet.
But what about shotguns?
Some medics take shotguns, and it’s not a bad idea because you have a number of places you can carry ammo. Shells fit in your helmet, 5 slot webbing, and all your regular pouches.
Additionally, shotgun ammo is more common to come across vs SMG ammo and fits in smaller places than M41A mags do.
Some medics take M41A MK1 or Heavy Pulse Rifles because those hold 100 or 300 rounds per mag respectively.
I don’t take these since medics aren’t fighters, I let fighters take these guns.
Some medics take the M10 pistol, not with any intent to kill, but to scare off xenos. Because it’s a lot of bullets flying, young and solo xenos may be warded off. However, any xeno with any sense of their health till close the distance, and stay however long he wants.
Protecting YOUR life
DO. NOT. DIE. YOU MUST live so others can be saved. This means you MUST have phenomenal situational awareness. I took a bit of a break from playing medic and wow do I make the dumbest situational mistakes.
Play it safe, and you’ll play it well.
- ALWAYS go back into cades.
- ALWAYS roller bed down marines to move faster.
- ALWAYS fallback with what you can grab in a retreat ON the call. Get a couple marines to go with you.
The hardest parts of staying alive are being behind the frontline after it pushes forward, determining when the frontline will collapse before it collapses, and getting to safety AFTER the frontline collapsed.
If no one is around, and you DON’T have “Medic cades,” it may be best to drag patients to the FOB, or forward to the front. Stop treating halfway, and roller bed your patient there. Be safe, NOT sorry. A collapsing front is surprisingly safer than a lonely backline. Riflemen can help take aggro off of you, or even scare off xenos chasing you down.
If you keep a close eye out, if you see 2+ T3 breaking through the last cade line on a flank, the front is going to collapse in less than 2 minutes unless 30% of the front rotates in that time. Call it out. If people aren’t starting to move in 30~45 full seconds, you may want to pre-emptively position yourself in a good spot for the retreat.
AFTER the collapse… Stick with riflemen and STICK TOGETHER. Do NOT leave people behind, unless marines are TRULY dropping like flies. A slow retreat with 8 marines is a much safer retreat than a fast retreat with 16. They WILL pick you off one by one, and they ARE faster than you.
Roller bed who you can. Fight to RETREAT. Do NOT secure kills as medic. It’s too risky!
FOB Siege
These are the scariest situations. If the FOB is being actively sieged, and you are still way far outside, get to the most remote place you can hide and FIND A PHONE! Landline phones, and Radio Backpacks should both be capable of calling the Normandy Dropship.
Medevac yourself with the Normandy to get back to friendly forces. It’s the safest way back.
FOB Collapse
DO NOT go to the other LZ. Where do you think the xenos are going?
Hopefully, you have planned for this or the Normandy isn’t being run by complete idiots.
If you aren’t getting to the alamo, or the alamo is going to be compromised, MEDEVAC!
Find the safest cades left. Xenos usually penetrate 1 or 2 sides. Most FOB have at least 3 with at least 2 lines of barricades. Get into something fully enclosed, and CAS Evac.
If you ran away from the FOB and xenos didn’t see you, Run to a really good hiding spot, and CAS Evac.
I changed my loadout a bit and I now take two cas evac beds with me, just incase I lose one for these very situations.
Finally, just stay alive… The best tip I can give is to get an Emergency Injector. It’s slightly dangerous because if you use it, and pass out still alive, a rifleman may ALSO inject you with one, and then you’re fucked.
The easiest way to get an “Emergency” or as I call it “!!” is to get ready normally. Get your pouches, your revive mix, your pads, your splints, IA, and whatever million other meds you don’t need from the pharmacy. (Looking at you, who ordered Tricordrazone pills. You know who you are, and the doctor rightly told you to buzz off.)
By this time, the REQ lines should be nearly finished, if not completely done.
REQ has “First Aid Pouch (full)” which is the Refillable Injector pouch in the middle vendor.
I leave the remaining injectors so REQ can toss it in a crate for grunts to restock on later.
Advanced Medic
Locating Incapacitated Marines
Technically they’re “dead” but they’re just in Cardiac Arrest. That’s why you can defib them. Just not “perma.”
First and foremost, yeah, just walk around, and be near the front. This works fine.
Marines will also bring bodies to you.
But for more advanced techniques, there’s a few strategies to make sure you find people not being found.
Pack something with an Optical Zoom.
- Binoculars
- Riflescope
- Flaregun
Binoculars are the simplest, and the most preferred method of looking out into the battlefield.
Riflescopes have 2x and 4x. The 4x can see the same distance as the Binoculars.This is a good way to save on inventory space, BUT you must be two handing the rifle to look through.
Flaregun. If you’re a pacifist medic, or using the General Utility belt on your armor slot, this sakes up the size of 1 rifle magazine. Pretty space efficient.
The best strategies are to look out into the battlefield, then the two flanks.
Forgotten bodies are also something to be concerned about.
People will drag bodies backwards behind friendly lines, and leave them there.
Every now and then, just peer back into your own lines. Someone could have been forgotten.
Nooks and Cranies.
Especially on the front, xenos like to trap marines into dark corners of small rooms.
Look in all the stupid rooms and dumb idea places to go. Marines aren’t smart. They just… walk into places, and die. They’re practically cave divers.
Body Recoveries
Recover dead and wounded bodies, but don’t give xenos yours.
gauge the chokes, and use HEDP if you need it to push a body towards your team’s lines.
Coordinate with SG to have them cover you if you make a semi-risky move if you KNOW you’re unlikely to get memed hard.
Before you leave barricades, Tell the riflemen to NOT follow you, and to stay away from the barricade doors.
Many riflemen will blindly follow anyone advancing, not stand off to the side and will stay on grab mode. Shooting these marines in desperate retreats may or may not occur. As a corpsman, it’s your responsibility to stay alive so you can treat any and all wounded marines that may or may not have been attacked by Xenos or panicked automatic rifle firing. In close-quarter environments, friendly fire often occurs as accidents happen.
Don’t get blocked. Make sure you can get out anytime you go in somewhere. If you’re unsure, don’t go in.
If you don’t have HEDP, see if a flamer is nearby, or if you have incendiary grenades.
Block the path for xenos with fire between the down bodies and the xenos so you can run in and recover the bodies.
UNLESS YOU NEED TO BE QUICK ALWAYS PICK UP THE GUN.
If you can pick up the gun, do so. If you need to be quick, forget about any gear. Other observers will get it, or the marine will get it if he’s able after he’s treated.
Some bodies will be on the outside of barricades and dead.
It’s often unsafe to recover these bodies by walking around to them.
Instead, what you can do is grab their body over/through the barricade and click on the tile you want to move said body to. This will allow you to move a body all the way to the door of the barricade safely so you don’t risk getting captured or killed.
Finally is FOB retreats.
Take SG or Medics on a roller bed if many troops are down.
Get out with one person, instead of dying with two. It sucks and you feel terrible leaving people behind. Especially if the guy you save is a bald SG or medic who DNRs.
Run safely, and yell at people to cover you.
Get out early, and take either the armor or the gun of your patient or just whatever gun or armor you see on the ground. If you have time or find a place where you can take a second to put it on your patient, do so.
It’s smartest to get to the FOB instead of treating the patient at all.
If you’re cut off by an OB, bunker down, run in the least predictable way that is neither towards friendlies nor towards the hive so you can hide.
Having radio backpacks helps because if the FOB retreat turns into an instant FOB siege, you may need to contact the Normandy for CAS Evac to get out.
Don’t lose your cas evac bed in an FOB siege because if the xenos breach south east, north west may be safe enough to cas evac the last few survivors before the cades fall.
Looting the Dead
You’re actually terrible if you don’t collect dog tags. So if someone dies, and you CAN collect the dog tag, by clicking the button in the bottom right… do it and keep it on you. Throw something away to store it.
You can stack information dog tags on top of each other without taking up more space.
Find some wood planks, and press Z to construct. If you have 2 you can make wooden crosses and place one dog tag on each cross. Make sure they’re somewhere safe, because if they get destroyed, those marines will not rest in flanders fields.
If someone is dead, you can remove the “shirt” to remove 90% of the gear. If they have a backpack, boots, and helmet, then those have to be removed separately.
If you have time to go through their stuff, toss out MREs, fire extinguishers, !! or “Emergency” injectors, splints, bandages, extended/ap mags, and grenades.
Try to make neat piles.
The other stuff is useful, but not as important for most marines, so you’re just making a mess.
put the empty bags into one pile.
Important bags to separate:
large magazine pouches, “spec” backpacks like rocket bags, spotter cloaks, radio backpacks, and large general pouches.
Pay extra attention to
This is a very hard skill to acquire, and is something you shouldn’t need to worry about until you’re at least platinum so you have the hard skills.
Flanks, and OBs. You ARE the last resort. If a flank is coming, you NEED to be aware of it so the wounded aren’t killed, and you are alive. As the medic, you have more social authority than most other marines because you save lives. Unless you suck. Most medics know who they don’t like and there’s only like 3 medics that are this. Most people that do medic are helpful players and therefore earned the situational awareness recognition of other marines.
If YOU say there’s a flank or you need to retreat, you’re more likely to get a detail to move how you need them to. Most non-brain dead SL and FTL will listen to medics.
Now OBs…
“Good hits” on our main force is something very scary.
You’re mostly supposed to be watching YOUR guys, not the enemy. If you know an OB is coming on your guys, call it out and RUN.
If an OB lands on your guys, you’re the only one who can save the few that can be saved and bring them to the FOB.
Dead CAS victims. There’s a glitch in the game right now where if you’re dead, THEN hit by CAS, you have insane pain damage. If someone is full health, and not getting up, they could be in extreme pain. I haven’t resolved one of these patients yet, but I assume painkillers may help.
OR…
sorry for the fucked up med scanner thing. I don’t know what I clicked that round.
They could be alive with 222 damage on their heart but still alive.
How? This spec blamed it on bad Unga from Research.

Don’t abandon patients just because they’re alive. Let them heal if you have others to tend to, but if everyone else is better, make sure the last people get up!
Questionable Ethics
Coming soon…
Unfortunately I forgot the medic that was getting into this…
Scattered Notes
Some subjects I wanted to cover included recovering blood from dead / perma marines to get O- blood. Looting near-perma marines whilst revivable in certain ways. And other various inhumane strategies that negatively affected individuals but boosted overall team value I no longer remember. There was some fucked up shit I learned but forgot in my 1~ year “break” from CM.
Loadout Brainstorming
Medic Specialties
There’s no “real” speccing like weapons specialists can pick RPG, Sniper, Scout, etc. These are “meta” specializations I have decided on and have no “real” existence of these specializations in the game. These are just “template loadouts” you can copy for inspiration.
General/Basic
Revival/Recovery
Anti-OD
Weymed At Home
Beginner / Basic
For a beginner, the “General/Basic” loadout is easiest.

You have all the important medical supplies in one spot. You can swap out the roller bed for the medical scanner to keep the scanner in your belt for ease of use.
This is sub-optimal, but it’s very simple and easy to use.
Put extra splints, medical scanners, and roller beds into your satchel or medical kit pouch.
Whilst you’re learning, this will just make it easy on you to learn.
The mags for your rifle are kept in your armor.
With the basic satchel you can access the items without waiting, and don’t have people calling you.
Revival / Recovery
The Revival/Recovery loadout is best for marines that are adept at recovering downed marines.
It’s best to take light armor with this loadout.



The radio backpack is used to call the Normandy for cas evac.
Inside there you can carry spare meds, extra HEDP, and a defib.
Flares are useful for seeing downed marines in the darkness and scouting dark tunnels for xeno presence to determine if it’s safe to recover.
In the medical kit pouch, you can take a bunch of roller beds. Roller beds take a second to setup, but are the fastest way to transport marines. Expect to lose of have your roller beds broken when running into enemy forces to recover dead.
Next is the drop pouch to carry 2 more defibs, and binoculars. Binoculars to look for dead, and defibs for extra revives.
I selected the M41A Mk2 as it comes with a 3 shot grenade launcher. This will let you carry 3 HEDP without taking additional storage. This offers you an instant way to fire HEDP to recover marines.
I recommend finding a way to carry a lot of splints. Perhaps by replacing some meds in the medkits in your backpack with splints or just putting splints into your belt.
Anti-OD
Anti-OD
When I started ODs were much more common, so I decided to learn medic without giving meds.
The core to this loadout is the lifesaver bag.

Storing 5 stacks minimum of trauma and burn pads allows you to swiftly treat any wounds without any doses of medicine. Because of how many pads you’ll go through, it’s good to take a few first aid kits. I take 3 and 2 defibs.
Just to keep things organised I keep my “advanced” medical supplies in the medical kit pouch.

Roller beds, spare med scanner, etc.
I may change things up but I currently put 3 hedp and my two blood bags into my 5 slot webbing, extinguisher, MRE, and scanner in my armor.
Weymed at Home
Finally is the Weymed at home.

Just taking one backpack can fit 7 medkits in your backpack. you can change out accessories as you need, but you can just take everything using the backpack, medical kit pouch, lifesaver belt, M4 armor.
If you want to, you have two hands, so you can take 3 total backpacks full of medical supplies.
Generally speaking, no one cares about the “oxygen” kits in medbay, so taking those supplies out to put the meds you want in them won’t bother anyone-unless you die with all the supplies on your own because you wondered off on your own.
My Personal Loadout
For those curious; this is my current loadout:

Helmet, usually have cigarettes in here too.

M4 armor. I’m adding the surgical kit today for IB.

drop pouch,

m39 rig, 3 extended mags, flashlight grip, reflex sight, bayonet

lifesaver bag, Just missing ia since it has to be made.

radio backpack, the 3 red kits are the same.

What’s in the kits in my backpack:


revival mix tricordizone,
medical kit pouch.

A few other fancy things I’ve seen other medics do:
Lysa Pierce uses Hypospray and Syringes with bottles, and vials. Not autoinjectors, but syringes.
Another medic… I can’t for the life of me remember who it is… he uses blood bags, takes the blood out, and puts meds into it.
And for the love of god… if I catch you using this loadout, I will come for you… Take IA DAMNIT!

Other Things of Note
Dickheads
Some patients will just suck and it doesn’t make any sense.

This was an instance of a marine that was nearing death close to T3s, no barricades, and a narrow hallway covered in weeds.
The patient had fractures, bleeding, and a lot of general damage, and I suspected the queen’s ability to come and screech with maybe 10 total marines in the general area unable to focus their force reasonably. I was dragging the patient out of the way of our friendly forces’ firing lines, and away from capture area. The patient deliberately resisted 3 times to break my dragging grip, and was complaining.
Some people don’t want to be helped even if they’re asking for help.
If a patient resists you 2 or 3 times, I would say it counts as refused treatment.
As a medic you have to be the one to decide “is this safe enough to treat a patient here?”
If not, don’t treat a patient there. You can’t risk yourself dying because some dickhead doesn’t want to walk 15 tiles back to where they almost died.
Does it annoy some marines if you take them 3 cade lines away, or a whole different building on the map? Yeah. But you need to decide for yourself “Do I feel like I personally am capable of treating this person in this environment?” Some medics can treat patients 4 tiles away from xenos without cades. Some medics take a whole minute to get their defib out.
It’s hard to manage all your items, your health, the health of your patients, the situation of enemy forces, and your teams ability to protect you. Whatever you need or decide is what you’ll do.
Take the North West Solaris Ridge LZ. If you’re fighting in the hospital, and you decide “I’m going to treat this patient inside the FOB” do it. Get your roller bed out, and take the patient there.
All you need is for a corner barricade to not have barbed wire, the front to get queen screeched, and a runner to capture you whilst your patient bleeds out helplessly.
But also be reasonable. Many players are new or simply don’t know anything of the medical system. Some marines will just walk away from you not knowing what you’re doing nor why.
Try to have patience. If they’re not talking, they could be deaf, not speak English, or tunnel vision. Grab patients and drag them where you want them. Patients walking away are not the same as patients “resisting.”
Some players are also just dicks. At least 3 different medics have explicitly told me, and NAMED NAMES of players they really avoid treating or will defib last intentionally.
If anyone is truly a dickhead, splinted, not bleeding, and alive is technically treated. If anyone “deserves” this, then that is the bare minimum if you wish to avoid specific people.
As a medic you should NOT do this to everyone and I think it would be considered against the rules, but if there’s like 1~2 players you really don’t like, this is fine.
Realistically you’re not going to tell the difference, but some players are very… verbose in berating your speed and even if you’re fast and some plat medics do say that’s why they under-treat some specific patients IF they have to treat them.
There’s 249 other players to treat, so if ONE is condescending, then move on.
Misc
Put your med scan window in the top right so it doesn’t cover chat, the main game, “view tac map” button nor the “show held item” button. I setup both of my health scanners before deployment, and close both windows. When I scan my next patient, the window will appear where I last put it for THAT scanner specifically.
NOTE: med scan windows cover other med scan windows. Sometimes the window for your active scanner is behind another med scan windows. Yes, that is annoying.

You can use middle mouse button click to open bags inside of bags without putting the “sub bag” into your hand. IE medkits in your backpack. You can even open them with your hands full.

Make sure you’re on help mode anytime you use a knife. Check for shrapnel by scrolling down on the med scanner just to be thorough. Some marines don’t know shrapnel is in the game and you can’t check for it by examining yourself nor checking yourself for wounds.
If you’re making incisions, holding wounds open, or treating IB, DO NOT MOVE, SWITCH HANDS, DROP ITEMS, NOR PUT ITEMS AWAY. It can and WILL cause further damage. The only exception is an emergency retreat. A small frac is not as bad as a marine passed out at the front after an FOB retreat call.
It is expected for you to have a fire extinguisher. The portable mini ones are in the lobby of medical next to the pharmacy. I recommend taking the safety off before storing it so you can instantly use it when you need it.
Finally is revival order.
RP dictates CO, XO, SO first and foremost… CIC deployers are annoying, and when those ones die, … anyway.
Medics always first. Why? Because if two medics are up, they can treat twice as many patients vs only one medic. And if you die, someone else can save you.
Com Techs second. Why? They can build barricades. stop the enemy from killing you whilst you’re healing marines.
SG is next because they’re the best fighter with IFF 900 rounds full auto.
Next is SL FTL, and spec because of their capabilities. The RPG spec may be worth reviving before the SG, but it’s very situational.
Last is Riflemen before survivors who aren’t Colonial Marines.
When surrounded by bodies and it feels like the whole world is on your shoulders and some fuck off spec with a single frac and for some reason zero splints is begging for medical attention over 5 orange flashing dead marines, the only thing you can say is “armor off” and try to position yourself between as many bodies as possible.
The best strategy I found is to defib everyone you can defib first, or treat with pads to defib. Don’t worry about their bleeding, fracs or anything. Just get them up first and say fracs and throw splints at them.
Save the easiest marines first. If they can make their recoveries, they can protect you, drag bodies, CPR, or even assist if they know how to.
In the case of an incin OB, pick one, maybe two marines if they’re next to each other. Fire extinguisher the heck out of them. Don’t run through THAT fire. make sure they’re not on fire. Strip armor, defib spam pad, and graft. Solo, you should be able to save one if you start immediately. If you’re really good, you can save two. CPR is important for marines to do if they are nearby.
Unfortunately the incendiary OB will likely stop being on fire BEFORE you revive the first marine.
HEDP can blast marines towards you and maybe even get them out of the fire to save more lives. Only save who you can.
Delta isn’t actually that bad. As Fizz found the joke about him funny, I’m sure you understand that my joke is not serious about Delta.
Conclusion
I went over a LOT of information. The two most important things to remember is to talk and ask for help; and the following Boondocks lesson:

“What do you do when you can’t do nothing, but there’s nothing you can do?”
“You do what you can.”
Just do what YOU can.
Some medics can treat 4 patients at once. Is that you? Awesome if it is, if it’s not you, do what you can.
I don’t think I missed much of anything new. I may tweak things here and there, and drop an update reply, but this should be good for at least a few months… I hope I didn’t overlook not updating some things.
A lot of things are the same since it’s just core medic stuff.
I mentioned only a few medics. I know there’s a LOT more solid medics.
wowza… high pop is 150 these days?
Since when is mid-pop 125??? Anyway… the game is balanced imo for 175~225 players.
Thusly rounds went from 2.5~3 hours down to 45 minutes ~1.5 hours… ![]() It’s really not the same.. what happened? Did A.S.S really do all-at? Or did enough of the valiant community members really dip along with those that looked up to them? This is fr breaking my heart.
It’s really not the same.. what happened? Did A.S.S really do all-at? Or did enough of the valiant community members really dip along with those that looked up to them? This is fr breaking my heart.